Outdated Policy, Modern Costs: Rethinking Pharmacy Choice in Workers’ Compensation

Cliff Goldstein litigated more than 1,000 occupational disease and other complex workers’ compensation cases while serving as the CEO and as a Senior Litigator at Chartwell Law, a top 200 national firm. Previously, he founded and ran Weber Goldstein, n/k/a Weber Gallagher, another large defense firm. He recently founded Outsource Consulting, offering strategic advice to employers, carriers and defense attorneys on the best strategies for handling high-exposure and complex cases.
For more than a century, workers’ compensation laws in most states have allowed injured employees to fill prescriptions at the pharmacy of their choice. The policy was grounded in a very different era of healthcare—one in which patients relied on close, personal relationships with local pharmacists to guide treatment decisions and improve outcomes.
When workers’ compensation laws were first written, most people obtained drugs from small, local, neighborhood pharmacies where a druggist or apothecary would create remedies on an individual basis, often selecting unique ingredients and using a mortar and pestle, while patrons bought sundries or enjoyed products from the soda fountain or luncheon counter.
The druggist knew patients by name and relied on long-term relationships, memory and familiarity to craft the best potions for each client. Choice mattered because care varied meaningfully from one pharmacy to another.
Over time, however, pharmaceuticals became standardized, mass-produced, mass-distributed and tightly regulated. The pharmacist’s role shifted from creating medications to dispensing them safely and efficiently.
Today, prescriptions are processed electronically, drug interactions are flagged by software, and clinical decisions are increasingly guided by data systems rather than personal familiarity.
At the same time, the structure of the pharmacy market has undergone a profound transformation. Independent pharmacies have steadily declined—more than 30,000 have closed nationwide—while large chains, big-box retailers, and online providers now dominate distribution.
Pharmacy Benefit Managers (PBMs) sit at the center of most transactions, controlling pricing, reimbursement, manufacturer selection and network participation.
The patient experience has changed just as dramatically. In many settings, pharmacists oversee high volumes of prescriptions with limited time for direct interaction. It has been reported that some pharmacists approve over 1000 prescriptions per day, spending as little as 2 seconds on each.
Much of the dispensing process is handled by technicians, automation, clerks, interns and centralized systems. The traditional model of personalized, pharmacist-driven care is now the exception, not the rule, particularly because, by definition, each injured worker filling a prescription has already consulted with a physician.
Most drugs are now dispensed by big-box stores like Walmart or Costco, national drug chains such as CVS, supermarket-based pharmacies or are sold by online providers.
Other than arguing over insurance reimbursement policies, co-pay amounts, or trying to find out why a drug is not being covered by the involved insurer, few patrons are having any meaningful interactions with an actual pharmacist.
Recently, patient control of pharmacy took a new twist with the advent of the “workers’ compensation” pharmacy. These mostly online and often national companies market themselves as specialists in comp drug claims.
Because of workers’ choice, instead of using one of the thousands of pharmacies in their PBM networks, workers can be steered by their doctors or lawyers to a workers’ compensation pharmacy.
Such pharmacies frequently accept prescriptions for claims that have not yet been deemed compensable, providing medications without upfront payment and assuming the financial risk in hopes of later recovery.
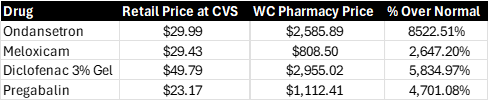
This business model drives a critical distinction: many of these pharmacies operate outside PBM networks. As out-of-network providers, they are not bound by negotiated discounts and often charge significantly higher prices to make back the potential losses on dispensing free drugs in contested claims. The result can be dramatic cost disparities for identical medications.
Compounding the issue, these pharmacies tend to dispense a disproportionate volume of high-cost, controversial products—particularly branded topical creams, gels, and patches that are clinically comparable to inexpensive over-the-counter alternatives.
In some cases, the price differences are not incremental — they are exponential. For example:
“Workers’ choice” does not always involve a workers’ conscious decision to use a particular pharmacy. Patients may be steered to certain workers’ comp pharmacies by lawyers or prescribing doctors.
Picking high-priced products from high-priced pharmacies may artificially inflate drug payments to engorge settlement amounts and increase contingent fees.
There are also case reports of financial interrelationships between some workers’ comp pharmacies and some prescribing doctors. It is unknown how much, if any, worker input is involved in the decision to use a workers’ compensation pharmacy.
 The original justification for unrestricted pharmacy choice — that patients benefit from individualized care and meaningful pharmacist relationships — has largely eroded. In today’s system, medications are standardized, dispensing is commoditized, and meaningful consultation is increasingly rare, regardless of where a prescription is filled.
The original justification for unrestricted pharmacy choice — that patients benefit from individualized care and meaningful pharmacist relationships — has largely eroded. In today’s system, medications are standardized, dispensing is commoditized, and meaningful consultation is increasingly rare, regardless of where a prescription is filled.
That leaves a fundamental question: does unrestricted choice still serve a meaningful clinical purpose, or does it primarily create an opportunity for cost inflation?
There are still arguments in favor of preserving patient choice. Some individuals may value continuity with a trusted pharmacist, and patient preference can play a role in adherence.
But these benefits must be weighed against the systemic costs—particularly when certain channels exploit the flexibility of the system to charge significantly higher prices.
A more balanced approach is available. Policymakers could allow employers and insurers the right to direct injured workers to pharmacies within established PBM networks — networks that typically include tens of thousands of locations nationwide — while still preserving broad geographic access and choice.
Alternatively, states could maintain open choice but impose a “usual and customary” pricing ceiling, ensuring that any selected pharmacy charges rates consistent with the broader market.
Workers’ compensation systems are designed to deliver necessary care efficiently and fairly—not to subsidize outdated assumptions or enable opportunistic pricing.
The notion that unrestricted pharmacy choice inherently improves outcomes is rooted in nostalgia for a bygone era of medicine. Legislators should revisit the benefits of patient choice of pharmacy and compare any such benefits to the cost to taxpayers and employers. &








